First: Your reaction to an odd situation was absolutely correct,
@BDWoody, as the cardiologic intervention proofed.
Some facts:
- there are acute infarctions by plaque rupture that make sudden subjective symptoms, no former stenoses needed
- there are progressive stenoses of the coronaries that make diffuse symptoms by getting closer and closer, until to infarctiation (as seen in this case)
- no matter what origin an infarct is, a re-opening within 8 hours of the vessel saves heart muscles from dying, so: time is muscle
Some symptoms:
- the 'real' heart-attack, meaning plaque-rupture with acute severe symptoms, involves: acute chest pain, left arm pain (not to forget chin an tooth pain), cold sweat and fear of death (and maybe dyspnoe): easy to detect and should in any case be case for ER
- the more subtile heart-attack, "don't feel quite right" with some pressure on the chest but "does'nt hurt" and that "breathtaking" thing will be gone the next days ...
- 'bad stomach' or upper abdominal symptoms can be sign of right-hearted MI. There are studies that recovered that male's infarcts ar predominantly left-hearted and under physical stress (Fussballweltmeisterschaft 4 times more MI for example), as with female there is psychic stress predominant and infarcts predominatly right-hearted what makes them more difficult to discover.
Some hints:
- worst case is cardiac fibrillation due to MI, and that means sudden need for resuscitation (and cardioversion), and Nobody should fear to do any harm to the patient to do this! If someone is (near to) death, no one can do any harm anymore, except doing nothing! Just press the chest as strong as possible (some crackles should not stop this, that's only ribs) and forget (you even would not think about it) about giving breath. F=90-100/min, that serves also for sufficient ventilation. NO FEAR.
Some predictive notes:
- main reason for atherosclerosis is life stye, including nutrition's alteration of whatsoever and physical whatsoever, or, in short, drink and eat and move or not will do some determination
Some sidenotes:
- cardiac surgery and invasive cardiology are in a race for best practice for years. If it was for myself do'nt know how to decide (besides valve reconstruction, this would go for TAVI).
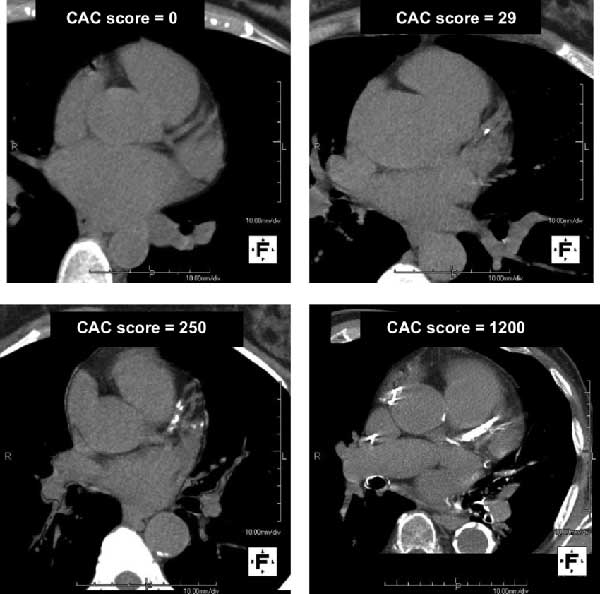
Some notes concerning radiology:
- there was Electron-Tomography a century ago to detect plaques
- GAF (Germa Airforce) uses Cardio-MRT to detect plaques
- Cardio-CT is now enforced to detect plaques
But this is all not predictive to determin risk for MI, and thus BS.
Some conclusion(s):
- Don't neglect severe symptoms
- Even respectable gears for home use (toys) may be misleading
- trust Yourself (unsiencely)
Recovery is in best progess, 'Call for humor' can't be missed. Same here.
Good luck.